NURS FPX 8022 Assessment 4 Quality Improvement Project Plan
Student Name
Capella University
NURS-FPX8022 Nursing Technology and Advanced Healthcare Information Systems
Professor Name
Submission date
Quality Improvement Project Plan
Patient safety and care quality are central to activities in the health services industry, and health information technology is an important contributor to this. Health information technology (IT) has the potential to enhance safety and quality outcomes by using information to support decision-making and reducing errors. The evaluation helps estimate potential benefits that could be achieved by leveraging performance measures when planning the integration of the barcode medication administration (BCMA) system and the clinical decision support (CDS) system into the Cleveland Clinic. Based on benchmark measures provided by the Leapfrog Group and the Centers for Medicare and Medicaid Services, together with the SAFER Guides framework, the analysis highlights the current gaps in medication safety, workflow, and the implementation of technology systems in the organization.
Problem, Significance, and Impact
While Medication Administration is a critical aspect of healthcare, it encounters numerous safety and operational challenges that profoundly influence patient outcomes and safety in today’s healthcare environment. Although progress has been made in improving safety, there is still a variation in safety performance across the organizations, highlighting issues with the use of health IT resources to improve safety performance. This is not confined to the Cleveland Clinic – performance measures identify issues with medication safety at the Cleveland Clinic. The problem is additionally affected by communication problems and poor patient experiences. The Leapfrog Group reviews patient safety data gathered by the Centers for Medicare & Medicaid Services and frequently reports that patients experience problems with understanding medication instructions and moving to a new environment. The complaints are tightly linked with the occurrence of adverse events at high rates among patients.
The issues can impact a number of stakeholders. These patients will be at higher risk for medication errors, resulting in potential for significant injury and decreased trust in the health care system. In contrast, the other side, that of the healthcare professionals, will suffer a greater cognitive load, lose productivity, and experience more errors due to the inefficient process and lack of appropriate technology. The BCMA and CDS technologies will address the root causes of the medication errors and will enhance the medication communications, thereby solving the problems.
Technology/Informatics Solution
One plan of intervention (solution) to solve the issues would be to implement the BCMA system as a full-scale project, since it integrates with the CDS functionality in the Cleveland Clinic’s EHR system. The BCMA will help to ensure that all five rights for each medication administered are verified during the procedure while using barcodes. The CDS function will assist in giving alerts when there are any precautions about allergies, drug interactions, and/or contraindications towards the use of certain drugs. When these technologies are integrated into advanced EHR software, like Epic, they can help enhance clinical decisions and avoid preventable medical mistakes.
Infrastructure improvements should be considered as a means of installing barcode scanners and reliable connections anywhere where there are patients. Second, there is a need to redesign the workflow to remove all the unsafe aspects of pre-scanning of medications and BCMA at the bedside. Third, optimization of CDS alert should come in tandem with the implementation of tiered alerting. Finally, training and competency programmes on the use of new technologies for staff would be important to consider. The proposed solution is directly related to the selected issue, and it addresses the underlying reasons related to the medication error and inefficiencies in the workflow. The process starts to get more accurate and efficient with the help of the proposed solution, and will also be compliant. In addition, the solution offers a way to generate valuable information to facilitate those changes to improve quality.
Monitoring Three Data Points
There are a number of data elements that demonstrate the need for and potential impacts of the initiative. For instance, it’s known that one of the primary causes of avoidable harm in the healthcare industry is medication administration errors, and this is presented in the Leapfrog Group. Poor performance in safe medication use is usual in hospitals, and these are generally not equipped with the appropriate technologies. Therefore, this is an area that needs to be addressed. The other set of data is from the Centers for Medicare and Medicaid Services Care Compare and reflects differences between customer satisfaction and performance. Cleveland Clinic has quite good clinical ratings; however, in terms of patient experience, especially regarding information related to medication usage, the results are not satisfactory. This can be addressed by integrating the BCMA and CDS–clinicians would have access to patient-related information.
Third, scientific studies prove the significant positive impact of BCMA and CDS applications on safety-related indicators related to drug administration. Also, the implementation of the BCMA technology can be expected to result in fewer medication errors and more medications administered as a result of verification obtained automatically, and in a lower chance of adverse drug events and better clinical decision-making processes. Hence, from the analysis of indicators, it is evident that there is a scope for improvement with respect to safety, communication, and process optimization. Furthermore, the data also demonstrate the sustainability of the proposed solution, as the data can continually be used to assess and improve processes.
Implementation Plan and Challenges
Logistics, human resources, and technology are all potential challenges with the implementation of BCMA and CDS at the Cleveland Clinic. In all patient receiving outpatient services departments, from a logistical point of view, it is essential to have readily available access to bar code scanners and system connectivity. If there are not enough technical resources, the process will be delayed, and other solutions will be used; this may impact patient safety. From a human resource perspective, there will be differences in the competence of both nurses and health care professionals to embrace BCMA and CDS, and the resistance to change.
Constraints on resources are yet another issue. Setting up BCMA-compatible infrastructure throughout all the outpatient areas and ongoing training and support for all employees and IT personnel can add up in cost. Also, security issues must be considered since this system will be able to be used for sensitive personal data, which is protected by the Health Insurance Portability and Accountability Act (HIPAA). Based on the risk management plan results, solutions to these issues are essential to ensure that the new technology can be safely and effectively implemented.
Leader Role in Change Management
The importance of leadership cannot be overstated in regard to successfully managing BCMA and CDS systems’ introduction to the EHR system at the Cleveland Clinic. Using sophisticated software is only part of implementing HIT in healthcare. Instead, requires a holistic change management and cross-disciplinary collaboration approach. Evidence shows that proactive leadership engagement in both the technical and social aspects of health IT adoption, such as involving professionals, communicating effectively, and changing workflows, is associated with successful adoption. As part of this, senior leaders, including CNO, CIO, and quality improvement representatives, will be tasked with formulating the big picture and identifying resources needed; ensuring all processes are related to the patient safety priorities. Priorities will be determined based on information about their clinical performance, to ensure the implementation of BCMA and CDS would improve efficiency and effectiveness, and meet regulatory needs. The Nurse Manager, Clinical Educator, and IT staff will become Change Champions to help implement the strategy in practice. Poor communication, low readiness, and trust can be key inhibitors of health care transformation efforts, according to studies, underscoring the role of proactive leadership involvement. Preparing an organization for EHR integration can involve recognizing strengths, such as the current state of the organization’s EHR infrastructure and its data analytics capabilities, and weaknesses that could impede integration, like issues with workflow alignment, hardware availability, or inconsistencies among staff competencies.
The eight steps of Kotter’s change model provide a process by which the transition can be facilitated. In particular, Kotter emphasizes the need to create a sense of urgency based on patient safety statistics, build a guiding coalition of leaders from a range of disciplines, and develop a vision centred on BCMA/CDS implementation. Leaders will have to continually communicate the vision, remove the barriers to transformation, including a lack of training and/or equipment, and achieve results rapidly, for example, better compliance with medication scanning. The implementation of new practices in the culture through policy and the evaluation process is referred to as change sustainability. Change sustainability involves embedding new practices into the culture through policy and evaluation.
Another key factor that should be addressed in relation to the implementation of BCMA/CDS at the clinic is communication. Communication must be ongoing during the whole process and feedback from employees should be in two ways – ongoing communication. Meetings and discussions may need to be at different levels to encourage communication with staff members. Staff meetings and other trainings, for instance, are examples of opportunities for leaders to communicate with staff. Meanwhile, information can be shared with staff online and even the highest echelons of management. The advantages of implementing BCMA/CDS and the potential for this to change workflow should be highlighted in each communication.
There are multiple aspects of a proper communication strategy. The principles are simplicity, regularity, relevance of information, and clearness. First, it is important to emphasize that messages should highlight the benefits that BCMA/CDS will provide. In order to ensure that the employees not only receive the change but also receive the skills they need for successfully implementing the technology, this training process needs to be included in the communication process. Leaders need to deal with resistance by understanding the roots and giving reassurance throughout the process of adopting change. In this regard, strong leadership and an appropriate communication strategy, backed up by a well-developed change management strategy, will definitely lead to success in adopting BCMA and CDS.
Communication Plan
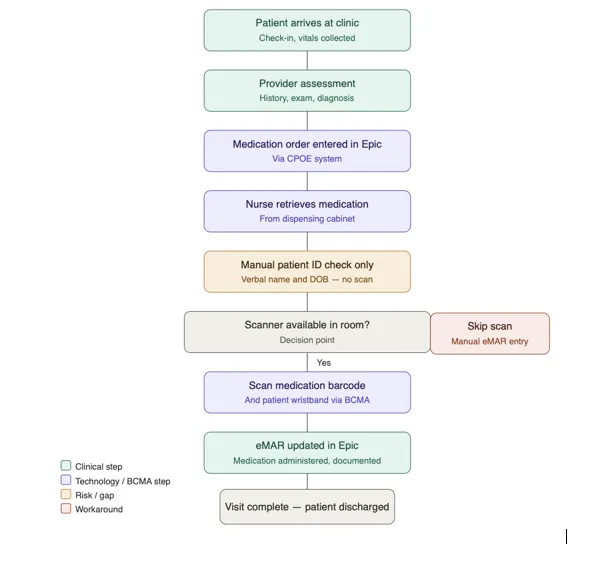
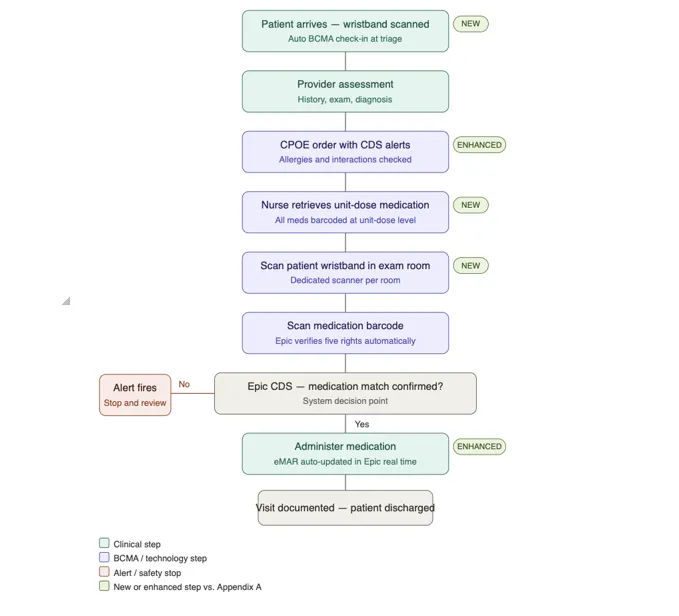
The communication plan needs to be customized for the implementation of BCMA and CDS at the Cleveland Clinic within the context of the new workflow design. The implementation communication plan will focus on ensuring clear communication about the alteration of workflows that will occur before and after BCMA and CDS are implemented. The pre-implementation workflows require a lot more human dialogue and elements for patients’ identification and medication verification, which places greater emphasis on human activities and poses risks of human errors and inconsistencies. Post-implementation, the workflow includes using technology, where nurses scan patients’ wristbands and medications using BCMA in conjunction with Epic and receive confirmation alerts whether patients’ medications, allergic reactions, and drug contraindications exist. As part of the process, the leaders will make use of visual depictions of the processes by presenting visual representations of the current state and future state of the workflows. These visual aids will be utilized to help everyone understand by presenting the facts in staff training and unit huddles. The following is a description of the post-implementation workflow. The post-implementation workflow is described in the following section, with a visual in Appendix B.
Workflow Analysis
The implementation of BCMA and CDS at the Cleveland Clinic requires the communication plan to fit within the framework of the redesigned workflow. The communication plan for the implementation will aim to provide clear communication regarding the changes in the workflows that precede and follow the process of implementing BCMA and CDS (Gordon, 2023). In the pre-implementation workflows, the process is highly dependent on human processes that involve verbal confirmation of patients’ identity and independent checking of medications, increasing the risks of human errors and inconsistencies. Post-implementation, the workflow involves the use of technology, whereby nurses scan both patients’ wristbands and medications using BCMA in integration with Epic and receive CDS alerts that confirm patients’ medications, allergic reactions, and any contraindications to drugs prescribed. As part of the process, the leaders will make use of visual depictions of the processes by presenting visual representations of the current state and future state of the workflows. Such visual aids will be used to facilitate understanding through presentations made in staff trainings and unit huddles. The visual of the post-implementation workflow is provided in Appendix B.
Summary: Final Recommendations and Conclusion
The adoption of BCMA and CDS will provide the Cleveland Clinic with an opportunity to make more strides in medication safety, reducing the likelihood of medication errors, and improving the quality of care. The SAFER Guides framework should be used for approaches to the implementation of the national performance measures and risk factors. Some of these elements of leadership, change management, and communication might help overcome the barriers to adoption.
Step-By-Step Instructions to write NURS FPX 8022 Assessment 4
For step-by-step instructions on NURS FPX 8022 Assessment 4, visit nursfpx8022assessment.com.
References for NURS FPX 8022 Assessment 4
Adeyemi, C., Adegoke, B. O., & Odugbose, T. (2024). The impact of healthcare information technology on reducing medication errors: A review of recent advances. International Journal of Frontiers in Medicine and Surgery Research, 5(2), 020–029. https://doi.org/10.53294/ijfmsr.2024.5.2.0034
Centers for Medicare & Medicaid Services. (2026). Find healthcare providers: Compare care near you | medicare. Medicare.gov. https://www.medicare.gov/care-compare/results?searchType=Hospital&page=1&city=Cleveland&state=OH&zipcode=44195&radius=25&sort=closest
Edemekong, P., Haydel, M., & Annamaraju, P. (2024). Health insurance portability and accountability act (HIPAA). National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK500019/
Gabutti, I., Colizzi, C., & Sanna, T. (2022). Assessing organizational readiness to change through a framework applied to hospitals. Public Organization Review, 23(1), 1–22. https://doi.org/10.1007/s11115-022-00628-7
Gordon, R. (2023). Why it’s necessary to improve team communication | American public university. Www.apu.apus.edu. https://www.apu.apus.edu/area-of-study/business-and-management/resources/why-it-is-necessary-to-improve-team-communication/
Heath, S. (2024). Patient safety improves as HAIs, medication errors go down. Patient Engagement; TechTarget. https://www.techtarget.com/patientengagement/news/366616012/Patient-safety-improves-as-HAIs-medication-errors-go-down
Jung, Y. Y., Walsh, Á., Patel, J., & Lai, K. (2025). Benefits and challenges associated with implementation and ongoing use of automated dispensing cabinet for medicines: A scoping review. Exploratory Research in Clinical and Social Pharmacy, 18, e100599. https://doi.org/10.1016/j.rcsop.2025.100599
Kotter, J. (2025). The 8 steps for leading change. Kotter. https://www.kotterinc.com/methodology/8-steps/
Laukka, E., Pölkki, T., & Kanste, O. (2022). Leadership in the context of digital health services: A concept analysis. Journal of Nursing Management, 30(7), 2763–2780. https://doi.org/10.1111/jonm.13763
Leapfrog Group. (2024). Sub-factsheet: Computerized physician order entry measure background. https://ratings.leapfroggroup.org/sites/default/files/2024-03/2024%20CPOE%20Fact%20Sheet.pdf
Leapfrog Hospital Safety Grade. (2025). Cleveland clinic foundation – OH – hospital safety grade. Hospitalsafetygrade.org. https://www.hospitalsafetygrade.org/h/cleveland-clinic-foundation
Malematja, D. N., Nkosi, E. M., & Nene, S. E. (2025). The impact of insufficient resources on the quality-of-service delivery at a primary healthcare clinic in Limpopo. Curationis, 48(1), e2696. https://doi.org/10.4102/curationis.v48i1.2696
Pettersen, S., Eide, H., & Berg, A. (2024). The role of champions in the implementation of technology in healthcare services: A systematic mixed studies review. BioMed Central Health Services Research, 24(1), 456. https://doi.org/10.1186/s12913-024-10867-7
Renukappa, S., Mudiyia, P., Suresh, S., Abdalla, W., & Subbarao, C. (2022). Evaluation of challenges for adoption of smart healthcare strategies. Smart Health, 26(1), e100330. https://doi.org/10.1016/j.smhl.2022.100330
Saleem, M. (2023). Barcode medication administration technology to prevent medication errors. Journal of the College of Physicians and Surgeons Pakistan, 33(1), 107–108. https://doi.org/10.29271/jcpsp.2023.01.107
Syrowatka, A., Motala, A., Lawson, E., & Shekelle, P. (2024, February). Computerized clinical decision support to prevent medication errors and adverse drug events: Rapid review. PubMed; Agency for Healthcare Research and Quality (US). https://www.ncbi.nlm.nih.gov/books/NBK600580/
Tansuwannarat, P., Vichiensanth, P., Sivarak, O., Tongpoo, A., Promrungsri, P., Sriapha, C., Wananukul, W., & Trakulsrichai, S. (2022). Characteristics and consequences of medication errors in pediatric patients reported to Ramathibodi poison center: A 10-year retrospective study. Therapeutics and Clinical Risk Management, 18(1), 669–681. https://doi.org/10.2147/tcrm.s363638
Williams, R., Kantilal, K., Man, K. K. C., Blandford, A., & Jani, Y. (2025). Barcode medication administration system use and safety implications: A data-driven longitudinal study supported by clinical observation. British Medical Journal Health & Care Informatics, 32(1), e101214. https://doi.org/10.1136/bmjhci-2024-101214
Appendix for NURS FPX 8022 Assessment 4
Appendices
Appendix A.
Figure 1
Visual of the Current Workflow
Appendix B.
Figure 2
Redesigned Workflow
Capella professors to choose from for NURS-FPX8022 Class
- Nicole Aclin, DNP, RN, CNE.
- Marylee Bressie, DNP, RN, CCNS, CEN.