NURS FPX 8022 Assessment 3 Risk Mitigation Plan
Student Name
Capella University
NURS-FPX8022 Nursing Technology and Advanced Healthcare Information Systems
Professor name
Submission Date
Introduction
It is important to use clinical decision support systems to support real-time evidence-based decisions, minimize medication errors, and improve safety, as these tools will help to improve decision-making processes. Although there are some instances in which it can be beneficial, CDSS can have some dangers as well. The risk mitigation strategy outlines how to mitigate the identified key risks that will be uncovered by the proposed integration of CDSS into the existing St. Francis Health Services’ barcode medication administration system, by applying the safety assurance factors for EHR resilience Guides. Every risk is also classified according to how likely it is to happen and the potential injury should it occur, and interventions are identified to keep patients safe, prevent health care failures and allow technology to be implemented properly.
Risk Mitigation Plan
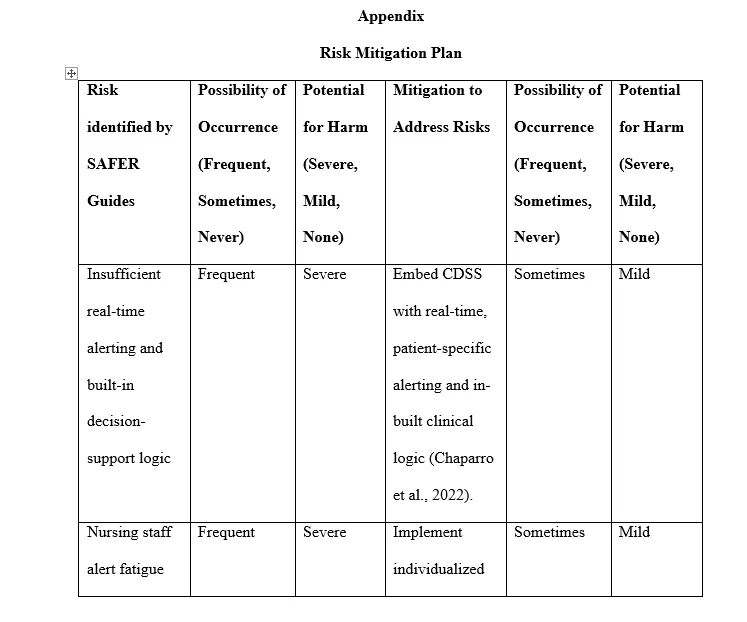
When evaluating the BCMA system at St. Francis Health Services for risk assessment of integrating the CDSS with the BCMA, there are a few areas that present risks. One big issue is real-time alert delivery to the clinical team and introduction of decision support logic; other instances might have more grave consequences. This gap limits the system to only being able to find high-risk medicine interactions and fall-related alerts, which cannot be easily identified, and can lead to adverse patient outcomes. To counter this, a plan is being put in place that entails timely and accurate alerts based on patient-specific data to help clinicians with decision-making and prevent errors at the bedside. The plan will be drafted for added safety of medication use.
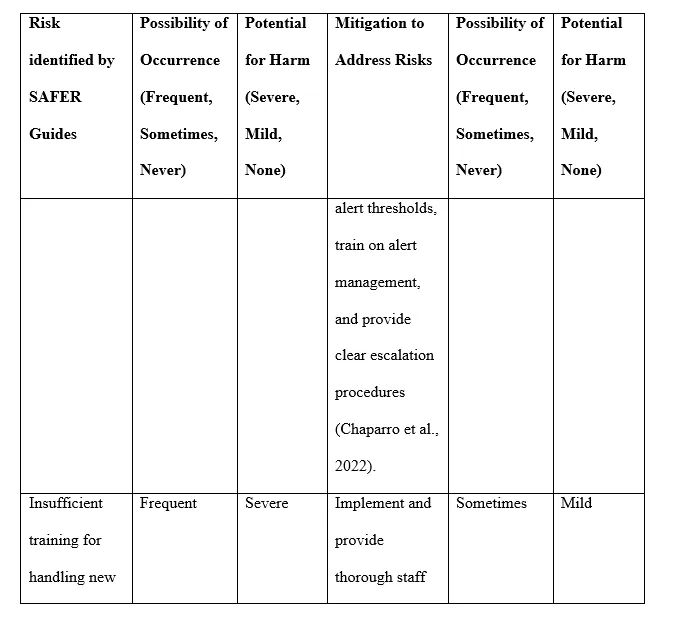
Another common risk is the “alert fatigue” of nursing personnel, even under normal circumstances, which may cause small harm, but could be a problem when it comes to the effectiveness of CDSS – increased risk that important alerts will be ignored or overridden. Nurses, at this stage, are not adequately prepared to deal with the various types of alerts, and this will only work with the right amounts and types of contextually-appropriate alerts that balance usability and safety. In addition, reconciliation issues with the data can occasionally occur, and can wreak havoc if there is not a proper synchronization of administration, medication orders, and actual medication administration.
Ethical or Legal Issues
If the risks outlined in this report for implementing CDSS in St. Francis Health Services are not addressed, there would be significant ethical and legal issues. Ethically, the safety of patients is the most important concern, and ignoring the risk of not having real-time alerts for medication orders, or a data contradiction in the medication administration record, could mean delayed treatment or medication errors, or an adverse drug event. The issue results in a breach of the ethical principles of beneficence and non-maleficence because patients could have been harmed by unnecessary system failure. Poor training in alert management can lead to the possibility of alert fatigue for the clinician (which can lead to a life-critical alert being ignored) and, over time, can lead to a loss of faith in the technology, resulting in moral distress or career implications to the clinician. As a result of the violation, patients can lose faith in the health care system and become less compliant with treatment and have poorer health outcomes (Vemuri et al., 2022). For not meeting patient safety and information protection requirements, institutions will be subject to fines and loss of reputation, and may even be held legally liable.
It is important to be aware that, in a legal sense, patient injuries or medication errors as a result of poor system protection could make the institution vulnerable to legal action, such as malpractice, regulatory action, and negative publicity. Healthcare organizations must ensure they deliver safe care environments, and technology that falls short of the standards could be in breach of the standards. Also, mishandling of patient information results in the breach of the Health Insurance Portability and Accountability Act (HIPAA), which demands sufficient confidentiality, data correctness, and access controls to protect patient data. Failure to abide by HIPAA could have serious consequences for the organization.
Unfortunately, the planned CDSS integration for St. Francis is not HIPAA-compliant because it does not include secure authentication, encrypting data while it is moving, or role-based access control to secure the availability of sensitive health information to only those who are appropriately authorized. Measures taken for cybersecurity are periodic auditing of the systems, availability of intrusion detection systems, designing the system properly, and also having a backup mechanism in case of any data leakage or if the system breaks down. The protections guarantee patient confidentiality and preserve the integrity and accessibility of clinical data, necessary for ethical and legal concerns. The institution takes proactive steps to protect patients, healthcare professionals, trust in the institution, and regulatory regulations.
Literature Justifications
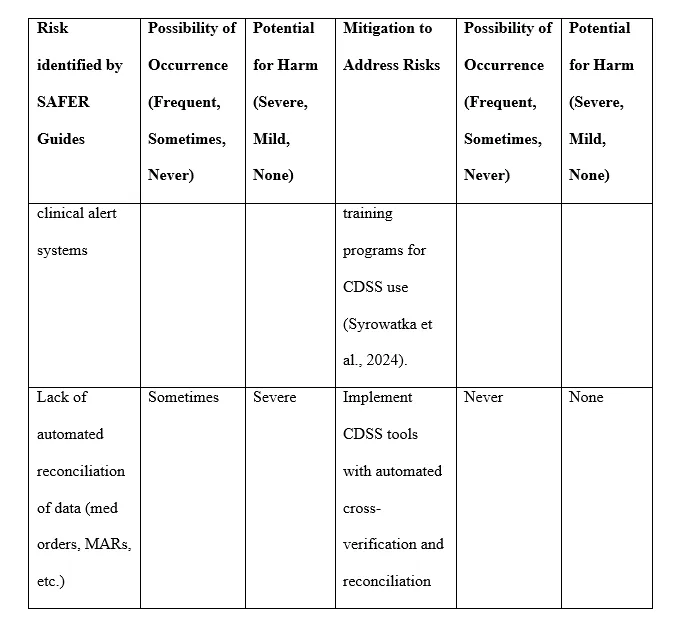
The proposed actions to address the risks found with the implementation of the integration of the Clinical Decision Support (CDS) System and the Barcode Medication Administration (BMA) System to St. Francis Health Services are logical in the context of good evidence and best practices in health informatics and patient safety. Real-time, patient-specific warnings are key to improving medication safety as they have been demonstrated to reduce adverse drug events and thereby improving clinical care. Then, when medication orders, administration, and patient charts are consistent and accurate, a common cause of medication error – automated cross-verification of data for data reconciliation – will be avoided. Finally, the method will decrease the chances of any discrepancies.
Evidence-informed flexible alert systems and ample education are used to manage alert fatigue: Too many or too generic alerts lead to desensitization among clinicians, the opposite of what is intended, and impact clinical decision support effectiveness. Responsiveness to alerts has increased while the number of alerts being ignored has fallen, thanks to part of clinician education and personalised alert thresholds, ensuring safer medicines management practices. Also, because of the extended training, the nursing personnel can perform the alerts correctly and react to them, avoiding risk due to cognitive overload and enhancing the care of patients.
These mitigation strategies follow evidence-based practice in trying to achieve a balance between sufficient clinical decision support, efficient patient safety maximization, and minimization of workflow disruption and cognitive load. How an organization takes a “path forward” approach leads to successful technology adoption and sustainment in healthcare organizations. Actions, therefore, recommended are not only directly addressing the known risk factors, but are based on current research consensus on how to optimize clinical results, and support health workers.
Change Management Strategies
In order to implement the recommended combination of CDSS and BCMA as well as mitigate identified risks from the SAFER guide, it is necessary to apply measures in the context of change management implemented towards goals. Frontline implementers for the St. Francis health services are the nursing staff, information technology support, clinical informatics experts, the pharmacists, and the administrative managers. Effective action needs to revolve around three main pillars – communication, involvement, and capacity development – to encourage effective and sustained practice change.
Kotter’s 8-step change model is one of the main strategies used, which begins with creating a sense of urgency to improve medication safety and clinical decision-making. First, the process begins with the reporting of Leapfrog safety scores and patient safety data to staff, to show the current gaps and how they need to improve. A guiding coalition of clinical champions (physicians, nurses, pharmacists) can help create buy-in and help lead the way on implementation. But it’s another key step: removing barriers, such as poor training or any disruption in workflow, by implementing targeted training programs and stepping up timelines as detailed in Kotter’s model – with the expectation of short-term improvements such as early signs of rate improvement with medication errors or end user satisfaction with CDSS alerts.
Another facilitative methodology that can be used is Lewin’s change management model: Unfreeze, change the current behavior to a new technology with adequate support, and refreeze the new behavior into routine practices. Under unfreezing, staff will be engaged using town halls or focus groups to consider present disappointments with manual medication processes. This hands-on learning and on-the-job assistance during the transition period will calm down the stress. Finally, refreezing accomplished by new policies and performance measures further solidifies the change for sustaining it over time.
Conclusion
Finally, this clinical decision support system with a barcode medication administration system is a smart, evidence-based approach to improve patient safety and improve clinical efficiency at St. Francis Health Services. The plan outlines a safe, effective, and sustainable transition through identifying and addressing threats with the guidance and SAFER Guides, as well as implementing change management strategies appropriate for the long-term care environment. If implemented correctly with proper risk management, ethical guidelines, and employee participation, the suggested technology is expected to enhance decision-making capabilities, reduce human errors regarding drug administration, and increase the overall quality of healthcare.
Step-By-Step Instructions to write NURS FPX 8022 Assessment 3
For step-by-step instructions on NURS FPX 8022 Assessment 3, visit nursfpx8022assessment.com.
References for NURS FPX 8022 Assessment 3
Chaparro, J. D., Beus, J. M., Dziorny, A. C., Hagedorn, P. A., Hernandez, S., Kandaswamy, S., Kirkendall, E. S., McCoy, A. B., Muthu, N., & Orenstein, E. W. (2022). Clinical decision support stewardship: Best practices and techniques to monitor and improve interruptive alerts. Applied Clinical Informatics, 13(03), 560–568. https://doi.org/10.1055/s-0042-1748856
Cremer, F., Sheehan, B., Fortmann, M., Kia, A. N., Mullins, M., Murphy, F., & Materne, S. (2022). Cyber risk and cybersecurity: A systematic review of data availability. The Geneva Papers on Risk and Insurance – Issues and Practice, 47(3), 698–736. https://doi.org/10.1057/s41288-022-00266-6
Edemekong, P. F., Haydel, M. J., & Annamaraju, P. (2024, November 24). Health Insurance Portability and Accountability Act (HIPAA). National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK500019/
Laka, M., Carter, D., & Merlin, T. (2024). Evaluating clinical decision support software (CDSS): Challenges for robust evidence generation. International Journal of Technology Assessment in Health Care, 40(1), e16. https://doi.org/10.1017/S0266462324000059
Laukka, E., Huhtakangas, M., Heponiemi, T., & Kanste, O. (2020). Identifying the roles of healthcare leaders in HIT implementation: A scoping review of the quantitative and qualitative evidence. International Journal of Environmental Research and Public Health, 17(8), 1–15. https://doi.org/10.3390/ijerph17082865
Miles, M. C., Richardson, K. M., Wolfe, R., Hairston, K., Cleveland, M., Kelly, C., Lippert, J., Mastandrea, N., & Pruitt, Z. (2023). Using Kotter’s change management framework to redesign departmental GME recruitment. Journal of Graduate Medical Education, 15(1), 98–104. https://doi.org/10.4300/JGME-D-22-00191.1
Miziara, I. D., & Miziara, C. S. M. G. (2022). Medical errors, medical negligence, and defensive medicine: A narrative review. Clinics, 77, e100053. https://doi.org/10.1016/j.clinsp.2022.100053
Rasool, M. F., Rehman, A. U., Imran, I., Abbas, S., Shah, S., Abbas, G., Khan, I., Shakeel, S., Hassali, M. A. A., & Hayat, K. (2020). Risk factors associated with medication errors among patients suffering from chronic disorders. Frontiers in Public Health, 8(1). https://doi.org/10.3389/fpubh.2020.531038
Stanz, L., Silverstein, S., Vo, D., & Thompson, J. (2021). Leading through rapid change management. Hospital Pharmacy, 57(4), 422–424. https://doi.org/10.1177/00185787211046855
Syrowatka, A., Motala, A., Lawson, E., & Shekelle, P. (2024, February). Computerized clinical decision support to prevent medication errors and adverse drug events: Rapid review. PubMed; Agency for Healthcare Research and Quality (US). https://www.ncbi.nlm.nih.gov/books/NBK600580/
Vemuri, N., Sneed, K., & Pathak, Y. (2022). Medication errors: An ethical analysis. Biomedical Journal of Scientific and Technical Research, 45(2). https://doi.org/10.26717/BJSTR.2022.45.007162
Appendix for NURS FPX 8022 Assessment 3
Capella professors to choose from for NURS-FPX8022 Class
- Nicole Aclin, DNP, RN, CNE.
- Marylee Bressie, DNP, RN, CCNS, CEN.