NURS FPX 8022 Assessment 1 Using Data to Make Evidence-Based Technology Recommendations
Student Name
Capella University
NURS-FPX8022 Nursing Technology and Advanced Healthcare Information Systems
Professor Name
Submission Date
Using Data to Make Evidence-Based Technology Recommendations
The concept of evidence based technology recommendations is imperative in the healthcare sector, as decision-making relies on data to assist a healthcare institution in understanding how to invest their money into technology which will directly translate to a patient and work efficient outcome in their care. By systematically examining the clinical outcomes, safety data and workflow factors, technology leaders can make informed decisions based on clinical data, rather than relying on vendor’s claims. The evidence-based strategy helps prevent implementation problems, ensure resources are used to their greatest extent, and ensures new technologies are connected to the quality improvement goals within the organization. At some point, innovations with measurable benefits and return on investment, and that offer better ways to deliver care, are adopted as a result of informed decision making. There will be a focus on the application of technology in real practice situations and use of performance information to generate technology advice, based on evidence in the assessment area.
Evaluation of Technology in Use
The Medical University of South Carolina University Medical Center (MUSC) has seriously underperforming with a fall rate of 0.774 per 1,000 patient days, compared with 0.000 for the Top performers, indicating there is a serious patient safety issue occurring at MUSC (Leapfrog, n.d.). The institution score on medication communication is 74 which is well below the top ranked hospitals with score of 88, indicating that there is lack of education to patients regarding their medication regime and side effects of the medicine they take. Incorporating strategic technology, combined with overall staff training programs, are crucial steps towards achieving perfection in patient safety and communication outcomes, and communication performance on discharge is on average below national standards (82) but better than other low performing facilities (67).
Patient education systems and medication dispensing systems that can be interacted with by the patients and medication that can be dispensed automatically can lead to a significant increase in medication communication and discharge planning in a healthcare facility. With the technological interventions, doctors will be able to provide the same trainings on the discharge and provide guidance on the medications with visual learning materials, on touch screen displays.The systems eliminate communication strategies differences and prescribe the systematic process of understanding patients’ adherence to medications and post-discharge care. Adopting technology solutions to standardise communication and medication workflow, will enhance patient safety and help to reduce the risk of preventable adverse events.
While the potential benefits of using advanced communication technologies in health care institutions are significant, the uptake of these technologies has been hampered by numerous barriers, such as institution related priorities, resource constraints and human issues within institutions when implementing. Patients’ education platforms are known for requiring staff to work harder and have limited experience with digital interfaces, which has raised a lot of opposition from staff. However, the process of buying automated systems for medication delivery and making investments in them to train employees, particularly by smaller healthcare facilities, is hindered by a lack of funds. Technological problems that occur when implementing the new communication platforms along with the current EHR systems can disrupt work routines and clinical functions of the old system. Navigating the touchscreen-based education systems could be a difficult task for patients who aren’t technologically literate, creating digital disparities in health care. In various health care settings, there are many central factors that make or break the success of health care technology implementation, such as planning and providing long-term administrative support.
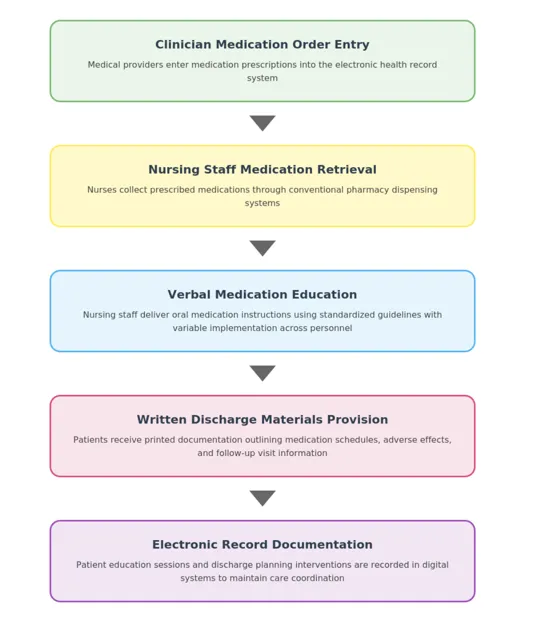
As is now, the MUSC’s existing medication communication/discharge processes include the involvement of the providers, who place the orders for medication in the patient’s chart, and the nurses, who receive the medication as instructed through the standard pharmacy delivery process. Nurses provide verbal medicine education in standardized education protocols; however this varies in quality based on individual nurses’ approach to the delivery of the information and time constraints. For efficient communication, there should be structured methodologies that would help in the various patient learning needs and preferences, particularly when delivery of patient education will be provided by a nurse using technology. The discharge instructions typically are provided to the patient in a written form, which includes a schedule of medication use, adverse effects and follow-up appointments. Documentation in the electronic health record system (EHR) ensures continuity of care by providing patient education contacts and discharge planning tasks that are sent to the EHR, generating lasting records. The present flow of the Work is given in Appendix A.
Patient Safety Areas Identified
Health facilities use two main assessment systems: Leapfrog safety ratings and Medicare assessment tools for comparing performance. In overall safety measures (e.g., adherence to protocols, infection control, clinical outcomes) Leapfrog assigns letter grades (A-F).Medicare compare studies so much more than the scope of aspects of the delivery of healthcare and satisfaction with regards to that, which makes it possible to study in the comparison to choose the provider. The three fundamental purposes of the evaluation systems are for transparency in operations, quality improvement systems, and to provide consumers with evidence-based information which they can use to make informed decisions about health care. The standardized monitoring frameworks are based on comparable assessment criteria and when combined, they help ensure a high-quality healthcare system that offers accountability and choice to consumers.
In the mentioned health care unit, the indicators of patient safety and communication quality exist and there are critical gaps in them. Medication communication scores (74) and discharge communication scores (82) are acceptable, but scores are not as high as those of the top facilities which are rated at 88 and 94, respectively (Leapfrog, n.d.). The discrepancies in performance provoke some basic questions about whether the medical center strives to develop a set of comprehensive standards of patient safety and provide evidence-based interventions in educating the patients.
Table 1
Medical University of South Carolina University Medical Center Score Comparison
Categories | Facility Score | Top Facility Score | Average Facility’s Score | Lowest Center’s Score |
Injuries due to Patient Falls | 0.774 | 0.000 | 0.338 | 1.748 |
Communication about Medicine | 74 | 88 | 74.64 | 59 |
Communication about Discharge | 82 | 94 | 85.48 | 67 |
Note. The data are a representation of Leapfrog safety grade ratings for the Medical University of South Carolina University Medical Center in comparison to the industry standards. The numerical results for the patient fall metrics are smaller the better the performance is, and the higher the score the better the performance is for the communication metrics.
The MUSC Medical Center has some strength in Medicare quality measures, as well as opportunities for improvement. An overall rating of 4-stars is achieved with 3-stars for the patient survey. The medical center has a very high level of compliance with influenza vaccinations (81% compared to 78% nationwide) and has strong performance in numerous infection prevention measures, such as central line-associated bloodstream infection (88% vs. 70% nationwide) and catheter-associated urinary tract infection (48% vs. 64%), but has not met expectations in sepsis (48% vs. 64%) or emergency department efficiency (88% vs. 92%). Results from the EDs show concerning delays, as the average visit in EDs is 216 minutes vs 195 minutes at similar high-volume EDs across the country (Medicare, n.d.). The results highlight important priorities for improving ED workflow optimization and sepsis recognition programs in the health care delivery system.
Operational performance figures for the healthcare sector reveal a significant variation in performance across withering healthcare verticals within academically strong medical institutes. Medication communication failures are present at Cleveland Clinic at a lower rate (57%), than at Mayo Clinic (66%) and both organizations experience difficulties with sepsis management at a lower rate (below the national average of 64% at 51% and 65%, respectively). The Cleveland Clinic had alarming metrics around how long it takes to see a patient in the ED with 196 minutes, whereas Mayo durations were longer at 203 minutes. Consider a difference as stark as that of compliance with influenza vaccinations, which are among Cleveland Clinic’s highest at 90% compared to the less than 78% national average and only 50% for Mayo Clinic. The Medicare Spending Indices are 0.94 and 0.99, respectively, compared with a median score of 0.99 across the census-tracts nationally (0.94 and 0.99 are lower than the national average – indicating fiscal stewardship variations for Medicare). Overall, it is clear that comprehensive quality improvement initiatives are still essential for improving patient care quality and efficiency in large healthcare systems.
Recommended Technology Implementation
To address these gaps in performance, MUSC should consider the use of patient education tablets that are interactive and automated bedside medication dispensing systems. Available evidence indicates that health care facilities with the integrated technologies had substantial improvements with regard to medication errors and to assist patients to understand their medications. Organization’s score in medication communication (74 points) and the rate of falls (0.774 per 1000 patient days) and the discharge communication score (82 points). The technology plan is fully compatible with the existing electronic health record infrastructure and meets specific gaps in patient education, access and safety across the health care continuum, making procedures for quality improvement easier. The automated feedback gathering systems in the form of touchscreen interfaces could streamline quality improvement procedures, and likely improve the overall satisfaction scores along the entire health care continuum.
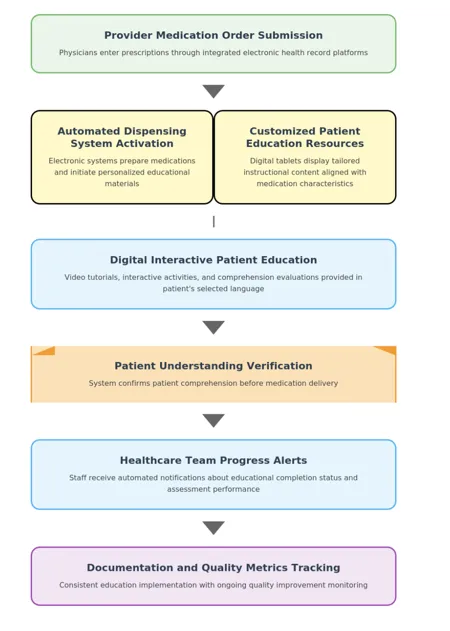
After the integration of technology, the medication management processes are changed to an interactive digital workflow, which enables the active involvement of the patients in the process of treatment encounter in place of the traditional verbal communication channels. Physicians order (via integrated computerized ordering systems), are notified of patient engagement levels before medication administration, with educational modules completed and assessment of patient knowledge results being displayed in the system; while the online platform offers custom video demonstrations, interactive simulations and comprehension testing in a variety of languages, chosen by the patients themselves. The safety measures entail a comprehensive education program and administration of the drug to the patient to verify that he or she understands how the drug is to be administered and what side effects it might produce. The method eliminates variability in communication, ensures that patient education is delivered in a consistent way and also establishes measures to monitor constant quality improvement. The simplified flow is shown in Appendix B.
Conclusion
One of the major approaches in an attempt to achieve sustainability in clinical excellence and efficiency of operation that healthcare organizations could use is inclusion of evidence-based technology. The result proves that automated medicine dispensation systems together with patient education electronic platforms, have a considerable impact on enhancing medication safety measures and communication protocols. By applying a systematic approach to the full scale quality measures used in the Leapfrog and Medicare comparison databases, the healthcare facilities will be able to identify performance gaps and make specific interventions with the technology as appropriate. The method enables the medical centers to fix some of the faults that exist in their operations; however, in quantifiable terms of quality improvement. Last, the tech recommendations based on the data result in sustainable changes within the quality of the care provided and patients’ satisfaction.
Step-By-Step Instructions to write NURS FPX 8022 Assessment 1
For step-by-step instructions on NURS FPX 8022 Assessment 1, visit nursfpx8022assessment.com.
References for NURS FPX 8022 Assessment 1
Altmiller, G., & Pepe, L. H. (2022). Influence of technology in supporting quality and safety in nursing education. Nursing Clinics of North America, 57(4), 551–562. https://doi.org/10.1016/j.cnur.2022.06.005
Bitomsky, L., Pfitzer, E., Nißen, M., & Kowatsch, T. (2025). Advancing health equity and the role of digital health technologies: A scoping review. BioMed Journal Open, 15(6), e099306. https://doi.org/10.1136/bmjopen-2025-099306
CMS. (2023, September 6). Hospital quality initiative public reporting | CMS. Cms.gov. https://www.cms.gov/medicare/quality/initiatives/hospital-quality-initiative/hospital-compare
Hickey, E., Man, B., Kaila, Lockhart, S., Duffecy, J., & Morris, M. A. (2023). Preferred communication strategies for people with communication disabilities in health care encounters: A qualitative study. Journal of General Internal Medicine, 39(5), 790–797. https://doi.org/10.1007/s11606-023-08526-4
Jungreithmayr, V., Meid, A. D., Bittmann, J., Fabian, M., Klein, U., Kugler, S., Löpprich, M., Reinhard, O., Scholz, L., Zeeh, B., Bitz, W., Bugaj, T., Kihm, L., Kopf, S., Liemann, A., Wagenlechner, P., Zemva, J., Benkert, C., Merle, C., & Roman, S. (2021). The impact of a computerized physician order entry system implementation on 20 different criteria of medication documentation—A before-and-after study. BioMed Central Medical Informatics and Decision Making, 21(1), 279. https://doi.org/10.1186/s12911-021-01607-6
Leapforg. (n.d.). Medical University of South Carolina University Medical Center – SC – Hospital Safety Grade. Hospitalsafetygrade.org. https://www.hospitalsafetygrade.org/h/medical-university-of-south-carolina-university-medical-center
Lyu, G. (2025). Data-driven decision making in patient management: A systematic review. BioMed Central Medical Informatics and Decision Making, 25(1), e239. https://doi.org/10.1186/s12911-025-03072-x
Mason, M., Cho, Y., Rayo, J., Gong, Y., Harris, M., & Jiang, Y. (2022). Technologies for medication adherence monitoring and technology assessment criteria: Narrative review. Journal of Medical Internet Research MHealth and UHealth, 10(3), e35157. https://doi.org/10.2196/35157
Medel, D., Bonet, A., Herrera, M. J., Sevilla, F., Vilaplana, J., Cemeli, T., & Roca, J. (2024). Interactive virtual simulation case: A learning environment for the development of decision-making in nursing students. Teaching and Learning in Nursing, 20(1), 60–68. https://doi.org/10.1016/j.teln.2024.08.002
Medicare. (2025a). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/100151/view-all?city=Jacksonville&state=FL&zipcode=&measure=hospital-timely-and-effective-care
Medicare. (2025b). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/360180/view-all?city=Cleveland&state=OH&zipcode=&measure=hospital-timely-and-effective-care
Medicare. (n.d.). Find healthcare providers: Compare care near you | Medicare. Medicare.gov. https://www.medicare.gov/care-compare/details/hospital/420004/view-all?city=Charleston&state=SC&zipcode=29425
Ong, B. N., Hodgson, D., Small, N., Nahar, P., & Sanders, C. (2020). Implementing a digital patient feedback system: An analysis using normalisation process theory. BioMed Central Health Services Research, 20(1), 387. https://doi.org/10.1186/s12913-020-05234-1
Osei, E., Asante, L. S., Wireko, S. A., & Abdulai, P. M. (2025). Digital health interventions for managing medication and healthcare service delivery by health professionals in Sub-Saharan Africa: A scoping review protocol. Digital Health, 11. https://doi.org/10.1177/20552076251379770
Pal, P., Sambhakar, S., Dave, V., Paliwal, S. K., Paliwal, S., Sharma, M., Kumar, A., & Dhama, N. (2021). A review on emerging smart technological innovations in healthcare sector for increasing patient’s medication adherence. Global Health Journal, 5(4), 183–189. https://doi.org/10.1016/j.glohj.2021.11.006
Provenzano, M., Cillara, N., Curcio, F., Pisu, M. O., Iván, C., & Herrera, M. F. J. (2024). Electronic health record adoption and its effects on healthcare staff: A qualitative study of well-being and workplace stress. International Journal of Environmental Research and Public Health, 21(11), e1430. https://doi.org/10.3390/ijerph21111430
Razick, D., Amani, N., Ali, L., Bachir, M., Salem, A., & Khatri, V. (2024). Leapfrog safety grades in California Hospitals: A data analysis. American Journal of Medical Quality, 39(5), 251–255. https://doi.org/10.1097/jmq.0000000000000200
Ricciardi, W., & Cascini, F. (2020). Guidelines and safety practices for improving patient safety.PubMed. Springer. https://www.ncbi.nlm.nih.gov/books/NBK585634/
The Leapfrog Group. (2023, November 3). New hospital safety grades from The Leapfrog Group find improved infection rates following major spike during the COVID-19 pandemic. Leapfrog.org. https://www.leapfroggroup.org/news-events/new-hospital-safety-grades-leapfrog-group-find-improved-infection-rates-following-major
Appendix for NURS FPX 8022 Assessment 1
Appendix A: Current Medication Communication and Discharge Workflow
Appendix B: Redesigned Workflow with Interactive Patient Education Systems and Automated Medication Dispensing
Capella professors to choose from for NURS-FPX8022 Class
- Nicole Aclin, DNP, RN, CNE.
- Marylee Bressie, DNP, RN, CCNS, CEN.